
I am Super Samson Simpson,
I’m superlatively strong,
I like to carry elephants,
I do it all day long,
I pick up half a dozen
and hoist them in the air,
it’s really somewhat simple,
for I have strength to spare.
~Super Samson Simpson – Jack Pretulsky~
My neck felt strangely tired and achy. I had just been for an afternoon walk and was now relaxing, watching the tennis. I struggled to heave myself out of the recliner. As I slowly stood up and stretched, I realised that I was unable to raise my arms over my head. I staggered to the sink for a drink of water, my hips refusing to cooperate by moving.
Even after almost two years since my myositis diagnosis, the sudden onset of weakness a few days prior to my IVIGs hits me like a truck. Within an hour, I go from blithely walking 2 km, leaping from chairs unimpeded, and even mindlessly rolling over in bed to having to calculate the effort required for each and every movement or activity.
Even sitting in a chair becomes exhausting, the effect of gravity dragging my head backwards, causing my neck and upper shoulders to protest this unexpected exertion. This sudden U-turn from being able to mop, dust, sweep, plan excursions, and live an active and useful life always resulted in a downturn of my mood as I was faced with being stuck in a sedentary life once more. After a relapse in June, where I spent more than four months struggling to walk, the PTSD of that experience was ever-present.
It felt like I had gone from easily hoisting an elephant onto my shoulders to struggling to carry a mouse. I did have hope though. My next infusion of IVIGs was only four days away….and they along with Myfortic would likely give me more than three weeks of being able to live a nearly normal life.
When I first became unwell with myositis, I actually had no idea how weak I was. I was shocked that I was unable to lift my legs off the examination table when the rheumatologist examined me. Over the next two years I slowly became an expert, tracking my weakness prior to IVIGs, and then my increase in strength after them. Over a period of months I would graph my ongoing improvement…or sudden deterioration!
My first improvements were subtle…though incredibly exciting to me at the time. After four weeks of treatment, the day I was able to touch the top of my head, and was in turn able to brush my hair, was almost earth-shattering. At this stage I was still in the dark as to how to increase my damaged muscles’ ability to move as I was unable to move at all. How could I exercise to get stronger when my hips and shoulders were essentially paralysed?
Eight weeks later, I had my first infusion of IVIGs, and 24 hours later, I was able to move my hips and shoulders for the first time in three months. It was now that I researched ways to measure my movement changes each month to document and accurately quantify my strength.
Just being able to move against gravity’s downward force was the first indication of my improvement in strength. This could be demonstrated by the ability to raise my arms over my head, lift my leg off the bed, and lift up my head when lying flat without a pillow.
But this was only the first step. The second step involved strength and endurance, not just the ability to move. Reading the literature, I found an excellent paper on monitoring shoulder and hip strength in myositis. This could be used to track the treatment’s efficacy and to detect any sudden deterioration.
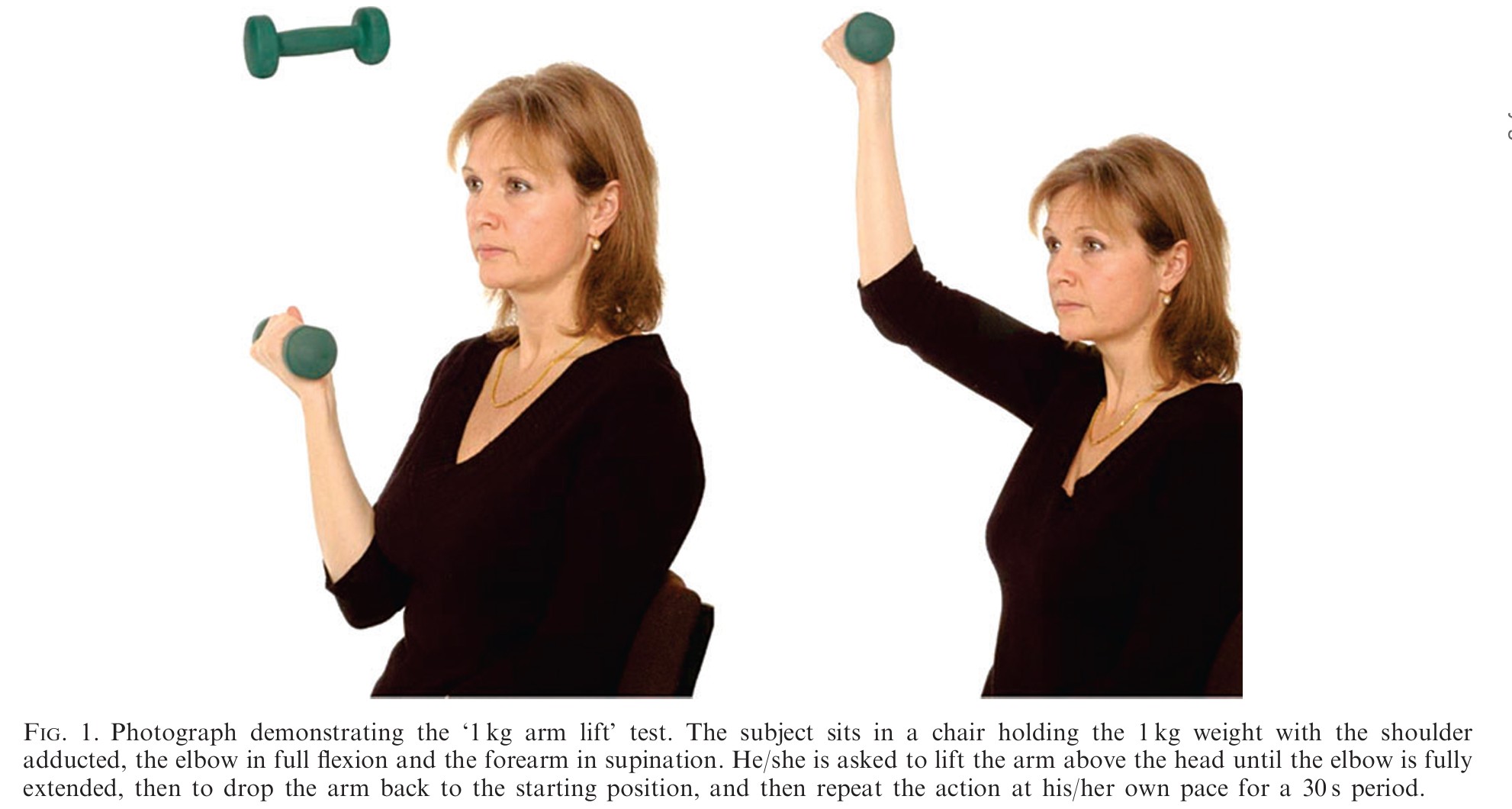
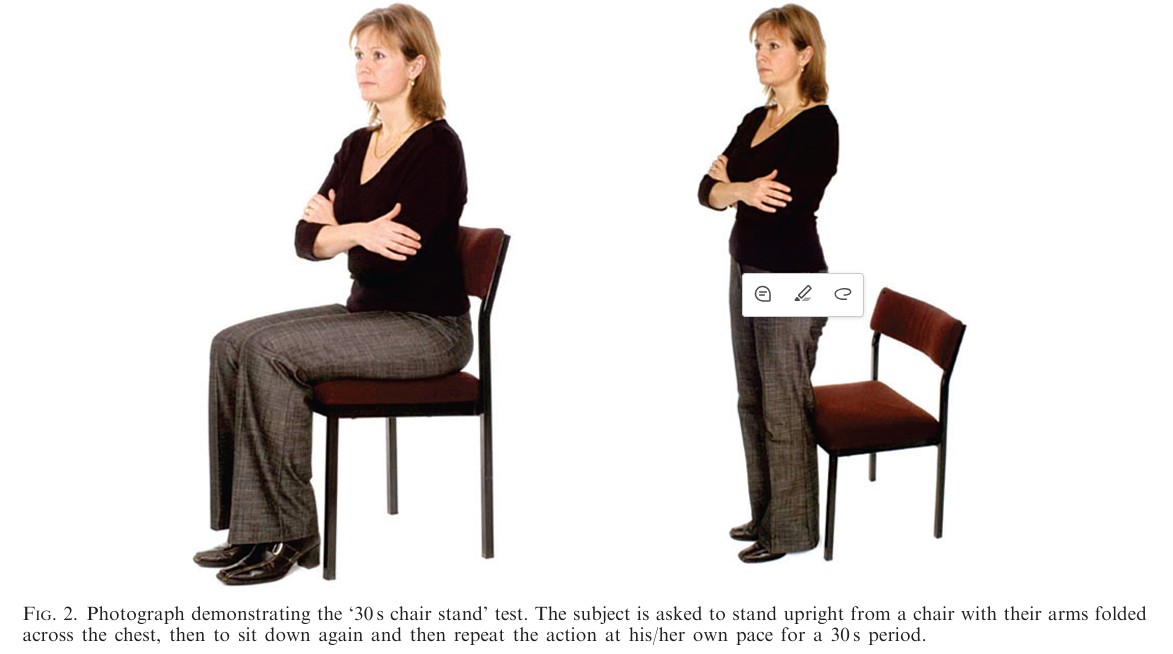
Every week I would measure how many times I could lift a one kilogram weight above my head in 30 seconds. I would then count how often I could go from sitting to standing with my arms crossed across my chest in 30 seconds. I could then track my strength over the months of treatment.
Another frequently used test is the six-minute walk test, which measures the distance walked in six minutes. I thought this might be useful when I was too weak to do the previous two tests, but could still do a slow, sluggish myositis waddle. However, I was walking so slowly that the fitness app on my watch refused to believe I was actually exercising! I figured if I could barely lift my feet off the floor, doing a 6-minute walk test was pretty pointless.
These at-home tests can give a better indication of what the physician will find when testing for strength in his office. Typically hip flexors (lifting the feet off the floor), shoulder abductors (moving the upper arms away from the body) and neck flexors (bending the neck forward) are tested as these are the weakest muscles in myositis. I can now describe to my rheumatologist the change in strength over the month and over several months.
As a patient we may describe weakness as fatigue or tiredness, not noticing the decrease in our ability to move our limbs against gravity, or our decrease in endurance. Rheumatology patients with many different disease processes often complain of fatigue as a major symptom, so this is frequently dismissed as something that can’t be easily fixed. It is often seen as something that the patient just has to learn to live with.
This is not necessarily the case in myositis, where muscle weakness is more likely due to poor disease control, especially when it rapidly worsens with decreased treatment. Because of this, it is important to be able to describe exactly how we are weak. It is often not recognised by our specialists the degree of disability myositis causes.
There are some specific types of myositis symptoms that can also be tracked. One of these is skin symptoms in Dermatomyositis. Other patients may have concurrent joint involvement. It is important to be aware that all patients are at risk of interstitial lung disease, but especially those with the Myositis marker Jo-1 and my Myositis-associated marker Ro-52. These patients should have yearly lung function tests and a high-resolution CT scan if they start to become more breathless on exertion.
Our oesophagus and bowel muscles can also be involved. Some people have obvious symptoms of choking on food and fluids. Some get typical reflux symptoms. A feeling of pressure in the middle of the chest after eating may be due to poor peristalsis, with food moving sluggishly into the stomach. Some notice voice changes due to weak muscles.
Another way to track disease activity and lung function is to wear a smartwatch and monitor daily steps. Some may not be aware of weakness and breathing problems, yet their daily step count unintentionally decreases. I find I go from easily walking 7000 steps a day to struggling to walk 2000 steps just before my next dose of IVIGs.
Specialists often focus on test results to gauge the likelihood of disease control. It can feel like a CK level is a black-and-white test… active myositis if it is high, and inactive myositis if it is normal. But this is not necessarily the case. Examining the patient and discussing what activities they are unable to do is often far more accurate.
Some key activities to document are:
1. Ability to lift feet when getting into the car
2. Getting dressed and undressed
3. Getting out of chairs
4. Getting out of bed.
5. Rolling over in bed
6. Washing and brushing hair
7. Reaching shelves
8. Walking downhill or on uneven ground
9. Ability to climb stairs
On the Myositis website, there is a myositis tracker that can be used at doctors’ appointments to describe the present degree of disability. Documenting weakness and other symptoms is important because it may indicate the need for more aggressive treatment. It can be frustrating, as we often know we are more limited than what a brief examination of our muscle strength provides. An astute physician will be aware of this and know how to assess both function and strength. However, there is insufficient time during follow-up appointments to fully assess endurance. One option is to see a physiotherapist or exercise physiologist prior to specialists’ appointments to document strength and endurance for our rheumatologist.
Lastly, there is fatigue. This is equally important, though different to weakness. One is systemic. One is purely muscular. Both can indicate disease activity, but only weakness can be measured. Fatigue, like pain, is reliant on the patient’s story. Rheumatologists find this hard to deal with. Most of their patients struggle with fatigue. Because of this, this symptom is often brushed off as unimportant. However, it is another important indicator of disease activity.
A recent study that interviewed both patients with myositis and rheumatologists found that patients were more concerned about fatigue, while Rheumatologists were more concerned about function. Even as a doctor patient careful to explain my weakness in terms of function, I felt that my rheumatologist heard only complaints of fatigue. It was, after all, what he heard all day, and every day.
You might have thought that at my follow-up rheumatology appointments, my specialist would have been pleased with my meticulous documentation of my progress. In fact, he usually looked at me like I was overly obsessed with my disease, and that if I just ignored my weakness, it would get better. He would look at me blankly and tell me that it made no sense. He had no idea why my strength could fluctuate so quickly before and after my IVIGs. (I have written about some of the causes of pain and weakness in myositis in a previous story.) What it did give me was the self-belief to fight for more and better treatment. I knew what I was capable of at my best, and therefore I knew when my myositis was still active.
Even as a doctor myself, I frequently found myself at a loss to explain my symptoms, as nobody seemed interested in listening to me. But believing in my ability to read my body gave me the impetus to argue and push back. I knew I was “probably” right! As a doctor, I knew too well the dangers of being too sure that you are right:) This danger many of my specialists seem to have lost sight of. Telling a patient that they definitely don’t have a certain illness often means that they will definitely have it! Both patients and doctors need to have the humility to listen to each other and make a plan. Lifting the heavy elephant of diagnosing and choosing the right treatment for a very rare disease requires both of us working together!
My muscles are enormous,
they bulge from top to toe,
and when I carry elephants,
they ripple to and fro,
but I am not the strongest
in the Simpson family,
for when I carry elephants,
my grandma carries me.
~Super Samson Simpson – Jack Pretulsky~
References:
- Two simple, reliable and valid tests of proximal muscle function, and their application to the management of idiopathic inflammatory myositis – Rheumatology 2006
https://acrobat.adobe.com/id/urn:aaid:sc:AP:87f2aae0-ec78-4c7d-ba81-2f616b373a21
2. Gathering patients and rheumatologists’ perceptions to improve outcomes in idiopathic inflammatory myopathies – Clinics 2022
https://acrobat.adobe.com/id/urn:aaid:sc:AP:cbca1615-33f8-463b-b896-83eddf063236
3. Questionnaire on functional capacity
https://acrobat.adobe.com/id/urn:aaid:sc:AP:987400f4-4830-4d61-b96d-47dc32eedf7c
4. A Valid and Reliable Functional Outcome Assessment Measure in Dermatomyositis and Polymyositis Patients. The Journal of Rheumatology.
https://acrobat.adobe.com/id/urn:aaid:sc:AP:8b60a221-6d20-4419-a902-302bd465a3b0
5. Scoring disease activity in myositis
https://acrobat.adobe.com/id/urn:aaid:sc:AP:5402203d-3cfc-4c76-9b55-d82254384c9f
6. Reliability of the Adult Myopathy Assessment Tool in Individuals With Myositis – Arthritis Care and Research 2014
https://acrobat.adobe.com/id/urn:aaid:sc:AP:1053e75e-dc81-4fa5-9651-3565f82f86c6
7. Fatigue as a common signature of inflammatory myopathies: clinical aspects and care – Clinical Experimental Rheumatology 2022
https://acrobat.adobe.com/id/urn:aaid:sc:AP:8e73d374-1d0f-48be-bc0f-a3fb130487d4
8. Quality of life in patients with myositis is associated with functional capacity, body composition, and disease activity—Baseline data from a randomized controlled trial – International Journal of Rheumatic Diseases 2024
https://acrobat.adobe.com/id/urn:aaid:sc:AP:118e53a9-424a-4b7f-b27d-801e9c8eec93
9. Patient insights on living with idiopathic inflammatory myopathy and the limitations of disease activity measurement methods –
a qualitative study – BMC Rheumatology 2020
10. My Myositis Tracker
https://acrobat.adobe.com/id/urn:aaid:sc:AP:0cc34274-ac39-4dae-bd39-6c9f9ed6b76c
11. Disease-specific quality indicators, outcome measures and guidelines in polymyositis and dermatomyositis H. Alexanderson, I.E. Lundberg – Clinical and Experimental Rheumatology 2007
file:///C:/Users/jctlg/Downloads/article-5.pdf/
12. Disease Activity Core Set Measures
https://www.niehs.nih.gov/research/resources/imacs/diseaseactivity
13. Making Patients and Doctors Happier — The Potential of Patient-Reported Outcomes – New England Journal of Medicine 2017
https://www.nejm.org/doi/10.1056/NEJMp170753
14. Manual muscle testing and hand-held dynamometry in people with inflammatory myopathy: An intra- and interrater reliability and validity study – 2018
https://pmc.ncbi.nlm.nih.gov/articles/PMC5875759/
15. Validation of Manual Muscle Testing and a Subset of Eight Muscles (MMT8) for Adult and Juvenile Idiopathic Inflammatory Myopathies – Arthritis Care Res 2010

thank you for this insight. I have recently been diagnosed with Inclusion Body Myositis. I’m 73 next month and have had the symptoms for over 2 years.
I am awaiting a referral to the Myositis clinic at the Royal Brisbane Hospital for ongoing treatment and management.
I am at present attending an exercise physiologist who has done a series of baseline measurements to track my progress/ decline. I was very pleased with that.
I have been doing water exercises nearly every day for the last 12 months.
I was informed that there is no cure or treatment for my form of Myositis, so I was interested to read you have treatment that seems to work.
I will speak to my specialist about it.
All the best,
Kathryn Campbell
Thanks for your comment Kathryn 🥰 I have Necrotising Myositis which is treated very differently to IBM. At the moment there is no known treatment for IBM but there are some clinical trials. The Myositis Association Australia can be a good source of information about these as well as good support. You are definitely doing the best thing with seeing an exercise physiologist. I’m in Northern NSW. All the best with your journey 💙